Rotator Cuff Surgery
Rotator cuff repair surgery is a critical surgical procedure for individuals suffering from rotator cuff injuries. The rotator cuff is a group of muscles and tendons that stabilize the shoulder and allow for a wide range of arm movements. When these tendons are torn, it can severely impact a person’s ability to perform everyday activities.
Several specialist techniques may be used to perform rotator cuff repair, each with its own set of advantages and considerations. Southern Orthopaedics’ specialist shoulder surgeon Dr Haber will advise you on the benefits and considerations of the suitable approaches for your specific circumstances and injury. For most, the key goals of rotator cuff repair surgery are to relieve pain, restore shoulder function and mobility, and prevent further damage to the joint.
A keen focus on postoperative care is crucial for a successful recovery. This typically involves physical therapy to regain strength and flexibility, as well as adherence to a rehabilitation protocol to ensure proper healing.
The information below covers what you need to do to prepare for rotator cuff repair surgery, what happens during the procedure and how to prepare for after the procedure.
Rotator Cuff Surgery – Before The Procedure
Booking In
Before the surgery, one of our staff members will discuss the date and preferred hospital you would like to attend. The hospital/day surgery units include hospitals in the North Shore, East Sydney as well as in the Illawarra region. We will prepare the booking forms for you to complete. Once a date has been decided, please book into the hospital as soon as possible via fax, email or booking online.
Please contact the rooms should you require assistance with this. When possible, please take the original booking forms that we have given to you to the hospital.
Preparation
It is important to wash your shoulder area with an anti-bacterial wash 48 hours before the surgery. This should be provided by the hospital when booking in. However, in some cases, you may have to obtain this wash from a local pharmacy. For the shoulder area, Benzoyl peroxide is the preferred wash as it reduces the Bacteria called C Acnes which can cause shoulder surgery infections. Make sure that when you apply the wash you keep it away from your eyes, lips and mouth.

Be prepared! Think about how difficult it will be with one arm completely out of action. You may need to purchase shampoo and conditioner with a pump pack and sometimes a scrubbing brush can be of some benefit. If you are responsible for your own meals think about preparing them before your surgery.
Medications
You must cease blood-thinning medications approximately 48 hours before surgery. These may cause excessive bleeding during surgery. There are several medications which can affect your body’s ability to form a clot. There are also non-pharmaceutical products that can have a similar effect. Please discuss this with your GP or specialist. We can advise you but we don’t want to interfere with directions given by your GP or specialist such as a cardiologist.
Be careful
Stopping blood thinners suddenly can be dangerous.
Always consult your GP or specialist before making any changes to these medications.
Blood-thinning drugs

Blood-thinning antiplatelet drugs include Clopidogrel, (Iscover, Plavix) and aspirin (Cartia etc). These need to be ceased about 7 days before surgery.
Warfarin needs to be ceased one week prior to surgery but may require a short-acting blood thinner to prevent the risk of forming a blood clot prior to surgery (this needs to be arranged through your GP or Cardiologist).
The newer agents such as Pradaxa, Eliquis and Xarelto only need to be ceased 48 hours prior to surgery.
Natural blood thinners, including Turmeric, Ginger, Cinnamon, Cayenne peppers and omega-3 fish-oil supplements, Vitamin E, need to be ceased 1 week prior to surgery.
Aspirin
To be advised by your G.P or specialist if it is safe to cease your aspirin. This must be done 1 week prior to your surgery.
Anti-inflammatory drugs
Nonsteroidal anti-inflammatory drugs (NSAIDs), Voltaren, Nurofen, Mobic, Naprosyn and Celebrex need to be ceased approximately 48 hours prior to surgery.
Fasting
You will be told by the hospital when to stop eating and drinking, however as a general rule if your surgery is in the morning fast from midnight otherwise nothing to eat or drink 6 hours before the operation.
X-Rays
Please bring any X-Rays, ultrasounds (except those from our clinic) and MRI’s you have into hospital with you.
Day of Surgery

Fasting

You will need to fast prior to your general anaesthetic. The hospital will contact you the day before surgery to discuss this with you.
If you have not fasted prior to a general anaesthetic, the procedure cannot proceed due to the risk of “aspiration”.
If you have prescribed medications to take while you are fasting you may take these with a sip of water unless instructed otherwise. You must take your blood pressure tablets when they are due irrespective of fasting. It is safe to take these with a sip of water.
Arriving
The hospital will inform you of the time you need to arrive. This is usually by a phone call the day before the procedure. Hospital operating rooms are on a tight schedule, so please leave yourself plenty of time and arrive early. If you have any problems please call the hospital as soon as possible.
The Pre-op. room

Once you arrive at the hospital on the day of surgery, you will be taken to the preoperative room and will get changed into a gown. Your shoulder will be cleaned with an antiseptic solution and covered by a drape and the shoulder will be marked. This is sometimes done in the operating theatre. Your anaesthetist, who is the doctor responsible for putting you to sleep and monitoring you during your procedure, will see you prior to the operation to check on your general health and readiness for the procedure. He will also discuss and prescribe the medications for pain relief following the surgery. He will then put a drip in your arm and make sure you are ready for surgery.
The Operation

You may not remember anything after the sedation is given to you. You are assisted onto the operating theatre bed. You will be placed on your side. You will then be completely anaesthetised and when you are asleep your arm is suspended in a traction device.

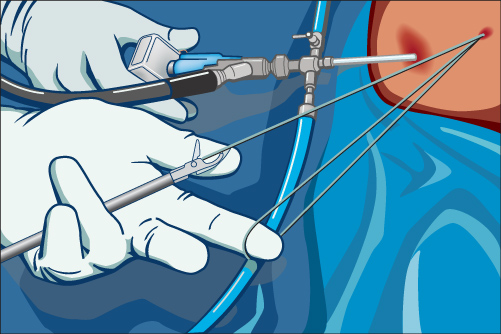
The procedure is done via “key-hole surgery” meaning it is performed through very small incisions (typically 4-8mm) called portals. Through one of these portals, an arthroscope is inserted to visualise the procedure. These are fibre-optic telescopes. A digital camera is then attached to the arthroscope.

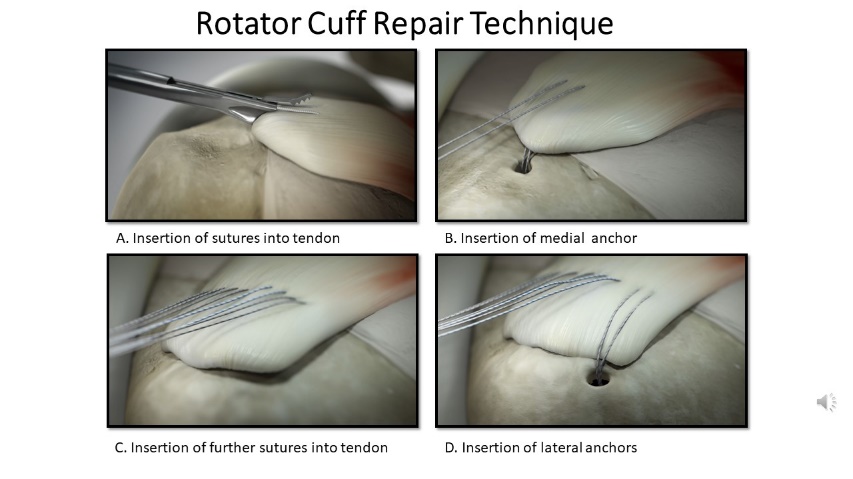
The details of how we repair the tendon through the portals are available on a separate video should you wish to watch. The procedure aims to reattach the torn tendon back to its bony attachment.
At the end of the procedure, the tendon is firmly attached to the bone.
Initially, therefore, the repair is entirely dependent on the hardware, that is the sutures and anchors.
Rotator Cuff Surgery – After the Procedure
Once the procedure is complete you will be transferred to the recovery ward When you are fully awake you may be discharged from the recovery room. We are happy to text your next of kin once the procedure has been completed. This needs to be organized prior to the day of surgery. If you opted for day surgery please ensure someone collects you from the hospital. You must not be alone for the first 24 hours after surgery. If you live alone you must have someone help with meals etc. If no one is available please let us know and we will organize for you to stay overnight in the hospital.

Going Home After Shoulder Surgery
Day Surgery Patients
You will remain in the recovery ward for approximately 2 to 4 hours. When you are fully awake you may go home.
Overnight Surgical Patients
You usually go home the morning after your surgery. Your follow-up appointment will be arranged prior to discharge.
The Dressings

When you leave the hospital, you will have two layers of dressing. A large bulky white dressing (combine dressing). This is removed 24- 48 hours following surgery prior to you taking your first shower (it is not a waterproof dressing and must not get wet)
There will be a waterproof dressing under the combine dressing. You may shower at this stage, but try and keep the waterproof dressing as dry as possible.
The waterproof dressings should, if possible remain intact for 5 days following surgery. If the waterproof dressings get wet or are starting to come loose, you may remove them and put a clean waterproof dressing on. Remember not to touch the inside of the waterproof dressing. You will have Steri-strips under the waterproof dressings. They may well come off with the waterproof dressings. If they are still on they will be taken off on your first visit to Dr Haber’s Rooms.

Following discharge home, there are a few things you will need.
We have included these in a pack. If you have not received prior to the surgery please let us know.

In the bag we provided, there is information about your surgery. There is also a dressing pack, a cold pack, a sling and a ball to squeeze for your exercises.
While we do provide some spare dressings, you may obtain more of these from your local pharmacy. It may be a good idea to take the packet to show them what was used.
We would strongly recommend a review by your GP approx. 3-4 days after the operation to discuss ongoing medications and review the dressings if needed. It would be worth booking this appointment before your operation.
Ice Packs
 Ice pack therapy helps alleviate pain following surgery. We recommend you place the pack over your shoulder for at least 20 minutes or until the ice has melted. You may need a spare pack that you can use while the other is freezing. A packet of frozen peas works very well. There are no hard and fast rules about how often and for how long you need to place the pack on your shoulder. Be aware ice packs are used to relieve pain and aid in your comfort so do what feels right for you.
Ice pack therapy helps alleviate pain following surgery. We recommend you place the pack over your shoulder for at least 20 minutes or until the ice has melted. You may need a spare pack that you can use while the other is freezing. A packet of frozen peas works very well. There are no hard and fast rules about how often and for how long you need to place the pack on your shoulder. Be aware ice packs are used to relieve pain and aid in your comfort so do what feels right for you.
Sling
 You will go home in a sling. The sling is only removed when you need to shower and remains on until your first post-operative visit with Dr Haber.
You will go home in a sling. The sling is only removed when you need to shower and remains on until your first post-operative visit with Dr Haber.
Sleeping
 Sleeping can be very difficult after surgery as it often was prior to surgery. You will generally be more comfortable sleeping as upright as possible and many people find sleeping in a recliner much more comfortable. Many people find it advantageous to rent a recliner for 4 to 6 weeks following surgery.
Sleeping can be very difficult after surgery as it often was prior to surgery. You will generally be more comfortable sleeping as upright as possible and many people find sleeping in a recliner much more comfortable. Many people find it advantageous to rent a recliner for 4 to 6 weeks following surgery.
There are 2 types of chairs. These include a Lift Chair and a Recliner chair. The Lift Chair Is specially designed to assist people after surgery and if mobility is an issue this would be preferred. It is electrically controlled which would be extremely advantageous especially if your right arm has been operated on and you, therefore, can’t use it if the chair has a lever on that side. The lift chairs can be rented from surgical/ independent living suppliers.
Your joints were made to be mobile and hate being kept still. I would, therefore, encourage you to passively move your operated arm into different positions. Try keeping your arm away from your body and you can rest your arm on your lap, the arm of the chair or a pillow.
I would strongly encourage you to keep your elbow as straight as possible for periods during your time out of the sling. If you keep your elbow bent upwards for prolonged periods at a time it puts unnecessary stress on the nerves in the back of the elbow (the ulnar nerve) which causes pins and needles in your ring and little fingers. It can also cause significant discomfort and stiffness of your elbow.
I would encourage you to keep your fingers, hand and wrist moving as soon as it feels comfortable after surgery.

It is not uncommon to develop swelling and stiffness of your hand following surgery. This can also cause pain and pins and needles in your fingers. It is also very helpful to continue to perform hand strengthening exercises as this prevents hand stiffness and general arm swelling as it aids the circulation in your arm. A stress ball or even a pair of socks works very well.
Problems immediately after surgery
Wound Discharge
As the procedure is performed by filling the shoulder with saline water, this may discharge through the portals into the dressings. If this leaks out of the dressings, the outer dressing may need to be replaced. A spare dressing will be given to you prior to discharge from the hospital. This discharge may be blood-tinged but is usually just the fluid with a little blood staining. Contact the hospital if it looks like the wounds are bleeding heavily through the dressings or the discharge does not settle within the first 12 hours.
Pain Management
Your anaesthetist will speak to you prior to the procedure to discuss appropriate post-operative medications. He will organise a prescription for your medications to control your pain as well as any nausea.

You should visit your GP four days after rotator cuff surgery for a repeat script before your medications run out.
Medication Side effects
You may be prescribed Celebrex or other Anti-inflammatory medications. These medications can upset your stomach. They are prescribed more for pain relief than their anti-inflammatory actions. Cease these medications if they are giving you trouble or are not providing any benefit.
Constipation
All narcotic pain medications can cause constipation. I would recommend eating a lot of fruit and visiting your chemist if you need further assistance.
Risks of Rotator Cuff Surgery
Modern techniques do minimize the risks of surgery, but cannot eliminate them completely. There are risks of general anaesthesia. These are EXTREMELY rare.
Specific to the rotator cuff surgery
The most significant risks of rotator cuff surgery include:
Infection
The quoted risk of infection is between 0.16% and 0.85%. Arthroscopic techniques significantly reduce the infection rates compared to open shoulder surgery. Preventative antibiotics are routinely given just prior to commencement of the operation. If infection occurs this may require further antibiotics and surgery. If you are feeling unwell or have developed a temperature please let us know ASAP.
Re-tear of the repaired rotator cuff
One of the most common problems after the tendon is repaired is that it fails to heal during the critical rehabilitation period, especially the first 12 weeks. Large, long-standing tears have very poor healing rates. Your age and health also have a significant effect on healing. We performed a study on this. In our patient population arthroscopic rotator cuff repair provides a significant improvement in functorial results in patients aged 70 years or older. Results are comparable if not better than in the younger age group. So if you are over the age of 70, don’t be put off. If we feel your rotator cuff tear is repairable, we anticipate you should have a good result irrespective of your age.
Compliance with the rehabilitation plan is critical. In one of the research projects, we found that if we obtain a good repair at the time of surgery the chance of the repair healing is nearly 95%. However, this drops down to only a 40% chance of healing if the patient was not compliant with the rehabilitation. We, therefore, stress the importance of complying with the rehabilitation we will provide to you.
Failure of the hardware
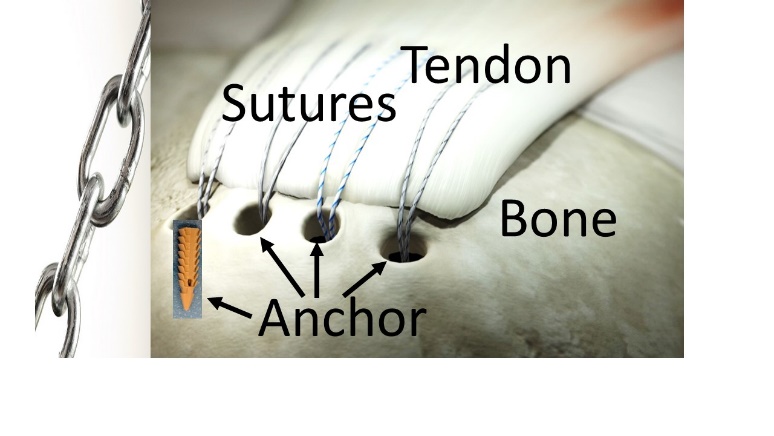
Initially, the repair is entirely dependent on the hardware, that is the sutures and anchors. The weak link (in the chain) can either be the tendon, the sutures, the bone or the anchors.

If you do too much while the tendon has not yet healed, either the sutures may cut through the tendon or the anchors pull out of the bone. We, therefore, stress the importance of carefully protecting the repair during the rehabilitation. Over time the bone grows into the tendons and the reconstruction no longer depends on the hardware. The timing of the healing and therefore the rehabilitation will be discussed at length below. If the repair fails to heal, further surgery may be required to re-repair the tendons.
Stiffness of the joint

Stiffness can occur after the surgery. It is almost always temporary but it may take 6 to 12 months to obtain your full range of motion. Ongoing stiffness after that period Is exceedingly rare (less than 1/20). Occasionally (approximately 3%), if the stiffness is severe, we can perform an arthroscopic release. Through tiny incisions (only a few millimetres) we can release the scar tissue which can markedly accelerate the recovery from the stiffness.
Smoking
Unfortunately, smoking can cause a number of problems following surgery. These include an increased wound infection rate, delayed healing of the tendon repair with an increased risk of re-tear. It can also cause other problems to your health including things like chest infections. We would therefore strongly encourage you to stop smoking at least six weeks prior to surgery.
Extremely rare risks of a procedure
There are some extremely rare risks of the procedure (<1/1000) that we need to mention. These include nerve injury which can cause permanent numbness and weakness.
The general risks of a procedure associated with anaesthesia are extremely rare. These include:
- Chest infection or collapse
- Clots in the legs or arm with pain and swelling.
- A heart attack. Death is an extremely rare complication from a procedure like this. The quoted figure from The Royal College of Anaesthetists is around 1 death per 100,000 general anaesthetics. That makes it rarer than being hit by a car as a pedestrian.
The recovery from rotator cuff surgery
For the first six weeks after surgery, only very gentle passive movement is allowed. You can commence gently actively moving your arm at six weeks following surgery. At three months you can actively use your arm against resistance and typically by six months most of your movement has recovered.
Initial Recovery
There are two important principles in the rehabilitation phase.
- Protecting the repair
- Preventing stiffness

Protecting the repair
The rotator cuff is repaired using stitches and plastic or metallic “anchors” which fix the torn tendon back on the bone. Initially, the success of the operation is dependent on the “hardware”. Over the subsequent twelve weeks, the tendon will knit onto the bone. Protection of the repair during this early phase of healing is therefore extremely important. Protect the repair by being careful not to use your shoulder actively, that is, do not lift your arm away from your side under its own power. Unless we tell you otherwise, you may use your hand for typing or writing as long as your arm is totally supported. You may rest your arm out of the sling supported on pillows for periods to let your skin breath. However, raising the arm actively, even a small amount puts excess strain on the repair and should be avoided. We will tell you how long these restrictions need to be in effect. During this time, you should leave your sling on when you are up and about and you should not drive!
Preventing stiffness
While your shoulder is healing, gentle passive motion helps prevent stiffness. Passive motion means that the shoulder is moved, but not under its own power. Your operated shoulder is moved by your other hand while the muscles of the operated shoulder are completely relaxed. At the first post-operative visit, we will show you how to do some gentle stretches and finger walks. You should perform finger and wrist exercises such as squeezing a ball several times a day. You can move your shoulder passively by standing up and bending over at the waist, allowing the operated arm to dangle down in a relaxed way (see diagram). Your good, non-operated arm can lift the operated arm which is relaxing, allowing the good arm to take all the weight.
Dos and Don’ts After the Surgery
Do
– Do wear the sling as specified, usually full time for 4-6 weeks.
– Do use your hand and forearm for eating, writing etc.
– Do perform finger, wrist, and elbow movements and hand strengthening.
Don’t
– Don’t actively lift your arm for at least the first 6 weeks.
– Don’t leave your sling off unless performing exercises or showering for the first 6 weeks unless specified.
– Don’t lift any weights above shoulder height for at least 3 to 6 months unless specified.
– Don’t drive for the first 6 weeks.
Phase 1: (weeks 1-6)

Overzealous movements, especially during the first 12 weeks, may destroy your repair.
You can continue to change your clothes and shower and wash even from the first day after surgery. This must be done with your operated arm remaining completely passive. Leaning forward, let your arm hang away from the body so that you are able to wash and dry yourself.
When getting dressed it is a good idea to wear loose-fitting cotton clothes which will help avoid a sweat rash. If you keep your arm directly against your body it can cause severe skin irritation. When getting dressed first place your top over your operated arm and then into your good arm.
You must wear your sling when you are up and about. However, when you are resting, I would encourage you to have your arm out of the sling, well supported, resting away from your body. This will help prevent a sweat rash. You can also straighten your elbow for comfort.
It is also critical that you keep moving your hand. It is not uncommon to develop swelling and stiffness of your hand following surgery. This can also cause pain and pins and needles in your fingers.
I would also encourage you to remain active as much as you feel comfortable. You should continue to take daily walks although the first two weeks you may find the pain will prevent you from doing too much. When you feel comfortable you can start increasing physical activity while always keeping your arm well supported in a sling.
I would like you to start performing some very gentle passive range of motion exercises after your first postoperative visit. You can perform gentle pendulum exercises. While changing clothes or showering you can lean forward so your arm hangs down. Lean over and you can use your good arm to support yourself on a table or chair. Relax the operated arm, letting it hang straight down. Let gravity gently move your arm away from your body. I would also recommend finger walk exercises.


Continue to use the stress ball or even something softer to keep your hands moving.
The second postoperative visit is usually at 5-6 weeks following surgery. At that visit, we perform a check ultrasound where appropriate. If there is no compromise in the repair you can come out of the sling and commence a regular passive range of motion exercises.
Phase 2: (weeks 6 – 12)

In the second phase (between 6 and 12 weeks) you can come out of the sling unless advised to delay this.
Dos and Don’ts
Do
– Do wean yourself out of the sling now unless specified otherwise.
– Do use your hand and forearm for eating, writing etc.
– Do attend your physiotherapist appointments and perform the exercises regularly.
Don’t
– Do not overdo your exercises.
– Do not lift any weights away from your body.
– Do not start any shoulder strengthening with weights or bands etc.
Physiotherapy
Formal Physiotherapy normally commences about 6 weeks after surgery, depending on the factors mentioned above. You should be given the physiotherapy protocol to take to your physiotherapist.
Precautions
– No lifting from the shoulder
– No supporting body weight with hands and arms
– No sudden jerking motions
– No excessive behind the back movements
Exercises

Initiate raising the arm without any resistance.
Gentle scapular and shoulder joint movements as indicated to regain full passive range of motion.
Continue ice as needed, may use heat before exercises.
Aqua therapy is good for light exercises.
Return to Activities

At 6 weeks after surgery, you may commence very light active use of your arm, that is, without any resistance.
You remain unfit for any manual duties using the operated arm.
You may start to drive an automatic car at this stage if you have achieved an adequate comfortable range of motion and feel safe. You are therefore fit for essentially clerical type duties only.
The ongoing rehabilitation depends on the severity of the tear and the risk of re-tearing. We, therefore, tailor the rehabilitation depending on the risk of re-tearing into low risk and increased risk.
Low risk
You may remove sling as tolerated, and eventually discard it.
Continue range of motion exercise with gravity eliminated and progressing to moving your arm against gravity.
Gentle moving your arm away from your body. Not against any resistance.
Increased Risk
You may remove the sling for increasing periods through the day as tolerated, and eventually discard it over the next 2 weeks.
Continue the range of motion exercises.
At about 8 weeks introduce gentle active movements not against any resistance.
Phase 3: Early strengthening (weeks 12-24)


At 12 weeks following surgery, resisted active use of the arm is now safe. You can commence light duties using the operated arm. There will however be significant restrictions using the arm above shoulder level and away from the body. At this stage, the shoulder remains very weak. Therapy includes continued stretching and you can now safely initiate a strengthening program.
Precautions
Sudden lifting or pushing activities, sudden jerking motions, overhead lifting Exercises.
Low risk
Work towards a full active range of motion. Continue stretching and introduce cuff stretching programme.
Begin resistance strengthening using bands and light weights as comfort allows.
Still avoid repetitive overhead use of the arm.
Increased Risk
Work towards a full active range of motion.
Continue stretching and introduce the full cuff stretching programme including posterior and inferior stretches.
VERY gradually begin resistance strengthening using Therabands between 14-16 weeks.
Avoid repetitive overhead use of the arm.
Gentle active abduction but no resistance work in this arc.
Phase 4: Advanced strengthening (weeks 24+)
Goals
Maintain full non-painful active range of motion.
Advanced conditioning exercises for enhanced functional use.
Improve muscular strength, power, and endurance.
Gradual return to full functional activities.
Precautions
Sudden lifting or pushing activities, sudden jerking motions, overhead lifting.
Exercises
Continue stretching if motion is tight.
Continue progression of strengthening.
Light sports (golf, tennis groundstrokes) can progress if your shoulder is comfortable.
At 6 months (24 weeks) following rotator cuff repair surgery, strong tendon to bone healing will have occurred and significant improvement in strength should have returned. At that stage, it is hoped you will be able to return to most normal activities.
By 12 months most people have made a full recovery from the surgery. You can return to preoperative sporting activities including such activities as training in the gym, playing golf and tennis and return to full manual duties at work.
FAQ
Why do I have a painful lump in my arm?
It is very common for people to notice a lump in the mid-arm region at 6 to 12 weeks following rotator cuff repair surgery. As pain following surgery does radiate down the arm patients are often concerned as to the origin of the pain and the lump. Let me reassure you all that the pain is referred from the shoulder joint. Surprisingly when we operate on the shoulder the pain is often worse in the arm than the shoulder itself. The lump you are feeling is the attachment of the deltoid muscle and tendon to its bony prominence which is called the deltoid tuberosity. It becomes more noticeable because of all the muscle wasting around the arm. It is, therefore, nothing to worry about.
Why is my shoulder still very painful and stiff three months after rotator cuff repair surgery?
Typically, the range of motion gradually improves after the first six weeks from when you start physiotherapy and by 12 weeks you may be starting to get a better range of motion than before your operation. Nevertheless, at this stage, there is considerable variation in the recovery of movement.
We did a study looking at recovery following surgery comparing pain and disability from preoperatively (before the surgery) to 12 weeks (3 months) and 24 weeks (6 months) following surgery. On average it took 12 weeks following surgery before pain and disability scores had improved beyond the preoperative state and by 26 weeks after surgery, patients saw substantial improvement. However, there is a huge variation in the recovery from surgery, especially at the 12 and 26 weeks reviews. When we correlated this with our ultrasound findings, we noted that the people who are feeling better in terms of pain and stiffness tended not to have healed as well as the people who were still very stiff and sore. In some ways, it is quite paradoxical. We postulated therefore that the ones who were more stiff and painful at 12 weeks following surgery (who we found were healing better) would ultimately gain better range of motion and strength compared to those who haven’t healed as well! We believe that people who have good healing form a lot more scar tissue around the repair and therefore tend to have more pain and stiffness.
So why do you get so stiff after rotator cuff repair surgery?
When we perform rotator cuff repair surgery we make an incision in the skin to go through the deltoid muscle, through the bursa to get to the rotator cuff tendon and then arthroscopically we then stitch the tendon back to the bone. Scar tissue can form between the skin and muscle through the bursa onto the rotator cuff. That scar tissue can restrict the shoulder motion. This is very different from a true frozen shoulder.
Is this stiffness at this stage following surgery a frozen shoulder?
You may be told if your shoulder is stiff following surgery you have developed a frozen shoulder. This can cause a lot of confusion. In the shoulder joint, you have the joint capsule and ligaments which give the joint flexibility. There is a condition we call a frozen shoulder where the capsule and ligaments become contracted and restriction in shoulder motion develops. This is a separate condition from stiffness following surgery.
In a frozen shoulder pain develops over a six-month period which can take 3 to 4 years to fully resolve. However, following a rotator cuff repair procedure, you are very sore after the surgery but the pain and stiffness gradually improve over 3-6 month and at 12 months is almost always fully resolved. A true frozen shoulder tends to occur in people sometimes between the ages of 40 to 50 but typically between the age of 50 and 60. It is rare after 60 years of age. It tends to be more common in women than in men. The age of the patient is the only thing a frozen shoulder has in common with post-operative rotator cuff repair stiffness.
What is the recovery from the stiffness?
At the 3-6 months mark, there may be a huge variation in recovery from surgery. We know that if the repair is intact at the three-month mark, it is going to be intact for many years to come. In a study we performed, looking at the long term (5 to 10 years) results of surgery, we found that there is consistent improvement, at the three months point to the six months and in the long-term pain and function almost always fully resolved. Be reassured stiffness at 3-6 months following surgery will resolve and you will consistently improve between the three-month, six-month and 12 month period. Usually, by 12 months, you have regained a full range of motion and strength and the pain has resolved. It will be well healed and hopefully, you will enjoy pain-free good function for the rest of your life.
Why is my hand swollen after shoulder surgery?
It is not uncommon (in nearly 30%) to develop pain, swelling and restriction in movement of the hand on the side of the operated shoulder following surgery. This typically develops over time and usually presents approximately four weeks following surgery. The cause of the swelling is not entirely understood but it is usually due to what is referred to as Shoulder-hand syndrome. This is often associated with finger numbness on the operated side after arthroscopic rotator cuff repair surgery and is usually very temporary. This is regarded as being a reflex “neurovascular” disorder meaning there is an abnormal reaction of the nerves of the arm because of blood vessel spasm. It is a reflex reaction to the shoulder surgery and is not meaning there has been any nerve damage. This is a reaction to what is called the sympathetic nervous system. This manifests with pain, swelling, and restricted movement of the hand and fingers and finger numbness. Other conditions that can cause very similar symptoms include Carpal Tunnel Syndrome (CTS), Cubital Tunnel Syndrome (CuTS) and flexor tenosynovitis (FT). This is only very rarely associated with a condition called a Complex Regional Pain Syndrome (CRPS) This is a clinical entity characterized by spontaneous pain that is disproportionate to the inciting event where movement limitations of the fingers and hand develop. The pain and swelling usually resolve at about four months following the shoulder procedure. I suspect this is because after three months you start to actively use your arm and this assists in the circulation of your arm which helps resolve the reflex “neurovascular” disorder.
When can I return to playing golf after rotator cuff repair surgery?
The rehabilitation, as well as the returning to sporting activities, needs to be varied based on a number of factors which may delay tendon healing. These include:
- large longstanding tears with significant tendon retraction or severe degenerative changes in the tendon.
- Diseases such as diabetes, medications, cigarette smoking, and being aged over 70.
The return to sporting activities, therefore, is not the same for everybody. I would not recommend any attempt at returning to golf prior to 12 weeks following surgery. Depending on the above factors, and if you are at low risk of cuff repair failure, I think it is safe to start gently playing golf at 12 weeks following surgery. Nevertheless, you must be careful handling your golf bag if it is heavy.
You can progress to chipping around the 16 weeks following surgery. By six months following surgery, you can return to playing a full game although it may take a few more months to regain good strength and range of motion.